
Syringomyelia (SM) Breeding Protocol
-
 2012 BVA-KC SM Protocol
2012 BVA-KC SM Protocol - 2024 Recommended Breeding Guidelines
- Conversion of 2006 Version to 2012
- 2006 SM Protocol
- Results of Following Protocol
- 2005 SM Protocol
- Related Links
- Veterinary Resources
The British Veterinary Association (BVA) and the UK's Kennel Club (KC) issued in March 2012 a set of Chiari-like malformation and syringomyelia (CM/SM) breeding guidelines*, with the aim of removing from breeding programs, cavalier King Charles spaniels with early-onset SM, and thereby reducing or even eliminating the incidence of CM/SM in future generations of cavaliers. In September 2012, BVA and KC slightly revised those guidelines. A current list of MRI-scanned cavaliers is available by clicking here.
* This SM breeding protocol is limited to cavaliers (and other breeds) registered with the UK's Kennel Club. The two USA national cavalier clubs have refused to acknowledge the existence of any SM breeding guidelines, and the US clubs place no restrictions on breeding cavaliers with CM/SM. See Editor's Note, below.
This breeding protocol replaces the 2006 SM breeding protocol which was approved by a panel of veterinary neurologists at an international syringomyelia conference. Click here to read that 2006 SM breeding protocol.
While the 2012 CM/SM scheme is open to all breeds, and particularly certain toy breeds and their crosses, it is no secret that CM/SM is largely a genetic disease of the cavalier King Charles spaniel, and but for the fact that nearly all cavaliers have CM and a vast majority of them have SM, the BVA and the Kennel Club would not have united to create this CM/SM scheme. See Syringomyelia for details of these disorders.
The CM/SM scheme requires that all dogs undergo one or more magnetic
resonance imaging (MRI) scans of
 the brain and upper spinal cord.
Records of these MRI scans and their analyses will be included in the UK
Kennel Club's Mate Select database program. This program is designed to
generate
Estimated Breeding Values (EBVs) for syringomyelia. EBVs are
statistical estimates of the genetic risk for a given disease of
individual dogs and a measure of the likelihood of passing the disease
on to their offspring. They are based on complex calculations such as
the prevalence of certain diseases in a particular breed and the size of
its gene pool.
the brain and upper spinal cord.
Records of these MRI scans and their analyses will be included in the UK
Kennel Club's Mate Select database program. This program is designed to
generate
Estimated Breeding Values (EBVs) for syringomyelia. EBVs are
statistical estimates of the genetic risk for a given disease of
individual dogs and a measure of the likelihood of passing the disease
on to their offspring. They are based on complex calculations such as
the prevalence of certain diseases in a particular breed and the size of
its gene pool.
An EBV can be calculated for most dogs even if they have not undergone an MRI scan, if they are related to dogs which have been scanned. Dogs too young for an MRI assessment can be assigned an EBV based upon the MRI results of their older relatives. See Estimated Breeding Values for more details.
Mate Select is intended to enable breeders to find more ideal mates for their dogs, in order to improve the health of future generations within the breed. It will allow breeders to assess the impact that a proposed mating will have on the genetic diversity of the offspring and maximize the chances of producing healthy puppies while also having the optimum impact on the breed’s genetic diversity.
While the use of EBVs and Mate Select are the optimum means of selecting mates for breeding CM/SM out of the cavalier, until the database for these means is front-end loaded with MRI analyses, the alternative for CKCS breeders is to follow the SM Breeding Protocol also devised by BVA and the Kennel Club.
The minimum age for a dog's MRI scan to be included in the CM/SM scheme is twelve months. There is no maximum age. For purposes of creating a most accurate EBV for a dog's offspring, ideally the dog should be scanned at five years or older.
A panel of neurologists and radiologists selected by the BVA will review each of the MRI scans. Two members of the panel will assess each scan, and if they cannot agree upon the grade given to the image, the panel's chief examiner will make a final decision. There is a procedure for appealing the panel's determinations, which is described below.
 The results of CM/SM grading will be sent to the submitting
veterinarian, who will forward the certificate to the dog's owner. In
addition the names and results of KC registered dogs will be sent to the
Kennel Club for recording on their database and made publicly available
on the KC’s database. The KC will forward the information to the Animal
Health Trust (AHT) KC Genetics Centre for inclusion in work towards
developing the EBVs.
The results of CM/SM grading will be sent to the submitting
veterinarian, who will forward the certificate to the dog's owner. In
addition the names and results of KC registered dogs will be sent to the
Kennel Club for recording on their database and made publicly available
on the KC’s database. The KC will forward the information to the Animal
Health Trust (AHT) KC Genetics Centre for inclusion in work towards
developing the EBVs.
To participate, the cavaliers' owners must sign a declaration certifying that the details are correct, and consenting that the results may be published in the Kennel Club's Breed Record Supplement and on the KC's website for use with its Mate Select program and for further research usages.
Appeals Procedure: The scheme grants the dog's owner a right to appeal the grade of the CM/SM assessment given by the BVA to the dog. The owner must file a written application for appeal within 45 days, followed by filing a certificate from the dog's veterinarian within the following 30 days, together with a re-grading fee.
 On appeal, the the MR images will be re-assessed by the Chief
Scrutineer, whose decision will be final, and the new grading result
will be sent to the Kennel Club for publication.
On appeal, the the MR images will be re-assessed by the Chief
Scrutineer, whose decision will be final, and the new grading result
will be sent to the Kennel Club for publication.
Beginning on July 1, 2012, the UK Kennel Club's Assured Breeder Scheme recommended that all CKCSs being bred first comply with the BVA/KC Chiari Malformation/Syringomyelia Scheme breeding guidelines. This is not a mandatory requirement for participants of the Assured Breeder Scheme. In 2016, the Kennel Club reported that that only 0.28% of cavalier litters registered in 2013 and 2014 have come from parents that have both been BVA/KC graded.
EDITOR'S NOTE: This SM breeding protocol may -- and should -- be followed by all cavalier breeders, everywhere in the world. The CM/SM Grading Scales (below) are a set of uniform standards which any veterinary neurologist or other veterinary specialist should use to grade any cavalier's MRI scan.
 2012
British Veterinary Association / UK Kennel Club Chiari Malformation /
Syringomyelia (CM/SM) Scheme
2012
British Veterinary Association / UK Kennel Club Chiari Malformation /
Syringomyelia (CM/SM) Scheme
CM/SM Procedure Notes
The BVA and UK's Kennel Club have issued a brochure intended to explain the Chiari malformation / Syringomyelia (CM/SM) Scheme and to provide instructions to those using the Scheme. It may be downloaded here in pdf format.
CM/SM Grade Scales
Chiari-like malformation (CM) is graded:
• CM Grade 0 = No Chiari malformation
•
CM
Grade 1 = Cerebellum indented (not rounded)
• CM Grade
2 = Cerebellum impacted into, or herniated through, the
opening at the rear of the skull (the foramen magnum).
Syringomyelia (SM) is graded:
• SM Grade 0 = Normal (no central canal dialation; no pre-syrinx*; no
syrinx).
• SM Grade 1 = Central canal dilation (CCD) less than 2mm in diameter.
• SM Grade 2 = Syringomyelia (central canal dilation which has an
internal diameter of 2mm or greater; separate syrinx; or pre-syrinx*
with or without central canal dilation.
The SM grade is followed by a letter (a, b, or c) indicating the age group at the time of scanning, as follows:
a = more than five years of
age;
b= three to five years of age;
c
= one to three years of age. The grade is not valid without the
qualifying letter.
* When viewing the MRI scan images for SM, a pre-syrinx, which is cord oedema, is sometimes seen. This may be transitional in the course of the progression of the disorder.
If the dog is not KC-registered or closely related to a KC-registered dog, then an EBV cannot be generated, and owners should refer to the breeding guidelines (below) and select breeding stock based upon the CM/SM grading result.
EDITOR'S NOTE: Notwithstanding the references on the above chart to breeding cavaliers as young as 12 months of age, the Mitral Valve Disease Breeding Protocol provides that no cavalier should be bred under the age of 2.5 years of age. Click here to read the MVD Breeding Protocol. Further, the OFA Hip Dysplasia Breeding Protocol provides that no dog should be bred under the age of 2 years. Click here to read the OFA Hip Dysplasia Breeding Protocol.
Downloadable copy of BVA/KC scheme: A copy of the BVA/KC's Chiari-like malformation /syringomyelia scheme is available here in pdf format for downloading and printing.
RETURN TO TOP
2024 Recommended Breeding Guidelines by Netherlands Researchers
 In
a
January 2024 article, a team of Netherlands researchers (Citlalli
Limpens, Vivian T. Smits, Hille Fieten, Paul Mandigers [right])
examined 2,125 cavalier King Charles spaniels in the Netherlands and
Denmark to evaluate the effect of MRI-based selection of breeding stock
on the prevalance of syringomyelia (SM) in CKCS offspring. Breeders
started screening their CKCS with MRI in the Netherlands since 2004, and
in 2011 the SM screening became mandatory. In Denmark, voluntary MRi
screening began in 2015, with mandatory testing beginning this year. The
goal of the study was to evaluate the effect of MRI-based selection in
breeding on the prevalence of SM.
In
a
January 2024 article, a team of Netherlands researchers (Citlalli
Limpens, Vivian T. Smits, Hille Fieten, Paul Mandigers [right])
examined 2,125 cavalier King Charles spaniels in the Netherlands and
Denmark to evaluate the effect of MRI-based selection of breeding stock
on the prevalance of syringomyelia (SM) in CKCS offspring. Breeders
started screening their CKCS with MRI in the Netherlands since 2004, and
in 2011 the SM screening became mandatory. In Denmark, voluntary MRi
screening began in 2015, with mandatory testing beginning this year. The
goal of the study was to evaluate the effect of MRI-based selection in
breeding on the prevalence of SM.
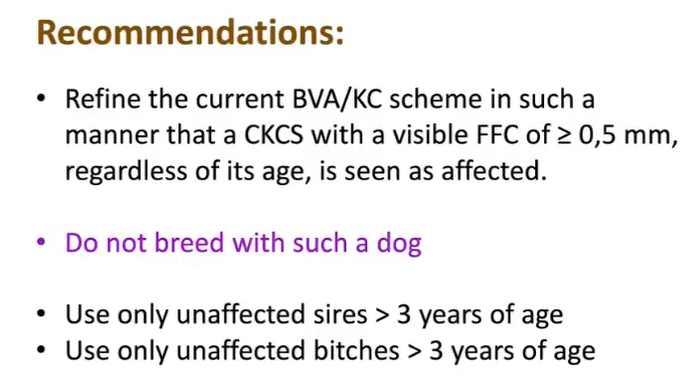
The researchers report finding that the prevalence of SM in the offspring of screened breeding stock decreased from 38.3% during the years 2010 through 2014 to 27% during 2015 through 2019. They found that breeding with both SM-affected parents significantly increased the risk of producing SM-affected offspring, compared to breeding with both unaffected parents. However, they concluded that "MRI-based screening and selection against SM led to a minimal decrease in prevalence of SM in the Dutch and Danish CKCS population." They make four recommendations:
1: Refine the current BVA/KC scheme in such a manner that a CKCS with a visible FFC (fluid filled cavity) of ≥0.5 mm, regardless of its age, is observed as affected.
2: Not to breed with such a dog.
3: Use only sires that are found to be unaffected after reaching the age of 3 years or older.
4: If possible, to apply the same to the bitches as well, only using them after reaching the age of 3 years and found to be unaffected at that time.
RETURN TO TOP
Conversion from 2006 Breeding Guidelines to 2012 Breeding Guidelines
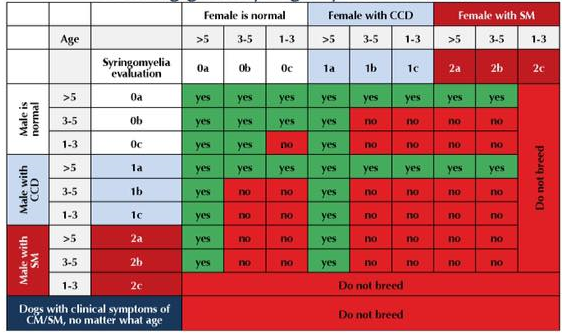
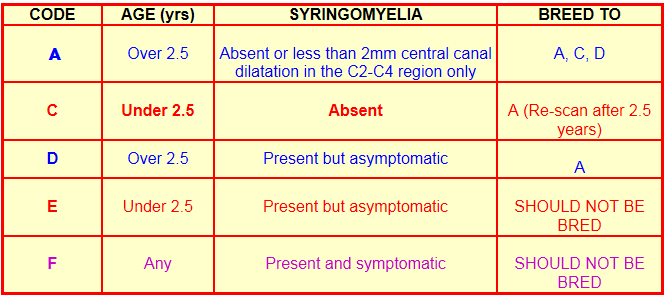
The chart below is to convert SM grades given to dogs under the 2006 SM Breeding Guidelines (i.e., A, B, C, D, E, F) to the 2012 SM Breeding Guidelines. The SM grade depends upon the age at which the dog was scanned.
Notes to the Chart below:
CCD = central canal dilatation
a = over 5 years
b = 3 to 5 years
c = under 3 years
Green = okay to breed
Red = do not breed
*A = dog over 5 years, no SM
# dogs with CCD aged less than 2.5
years were often attributed a D grade.
EDITOR'S NOTE: Notwithstanding the references on the above chart to breeding cavaliers as young as 12 months of age, the Mitral Valve Disease Breeding Protocol provides that no cavalier should be bred under the age of 2.5 years of age. Click here to read the MVD Breeding Protocol. Further, the OFA Hip Dysplasia Breeding Protocol provides that no dog should be bred under the age of 2 years. Click here to read the OFA Hip Dysplasia Breeding Protocol.
RETURN TO TOP
2006 Rusbridge Syringomyelia
Breeding Recommendations
by Clare Rusbridge, BVMS DipECVN MRCVS PhD
 Note: This is the SM Breeding Protocol which was in effect from
November 2006 to early 2012:
Note: This is the SM Breeding Protocol which was in effect from
November 2006 to early 2012:
Dr. Clare Rusbridge, BVMs, DipECVN, MRCVS, PhD., of the Stone Lion Veterinary Centre in Wimbledon, UK, published the following breeding guidelines in January 2007, for Cavalier King Charles Spaniel breeders to follow to try to avoid the worst aspects of Syringomyelia (SM) in future generations of Cavaliers.
Dr. Rusbridge and Susan P. (Penny) Knowler, BSc (Hons), have been conducting an extensive study of syringomyelia and the Cavalier King Charles Spaniel for several years, and they published their first recommended breeding guidelines for SM in January 2004.
In November 2006, at an international syringomyelia conference sponsored by the U.K. Cavalier King Charles Spaniel Club's research fund, the attending neurologists and other specialists from five countries conferred at the Royal Veterinary College in Hertfordshire to discuss revisions to the previously published versions of Dr. Rusbridge's SM breeding protocol. A result of that conference is this November 2006 protocol, the fourth version.
The aim of these breeding guidelines is to reduce the incidence of syringomyelia in future generations of Cavaliers, and to provide guidance until more information becomes available. An official British Veterinary Association (BVA) version of the SM protocol is expected to be published in the near future. Also the still under development Estimated Breeding Values (EBV) will enable breeders to better determine the relative breeding value of Cavaliers which rate an "A" under these guidelines.
This SM Breeding Protocol is not universally accepted by neurologists researching Chiari-like malformation (CM) and SM in the CKCS. Most significantly, George C. Skerritt, BVSc, MIBiol ,CBiol, DipECVN, FRCVS, of the ChesterGates Animal Referral Hospital in Chester, UK wrote in April 2008 that "I must comment on the breeding scheme recommended by Claire Rusbridge. In my opinion it is not nearly strict enough; it advocates the breeding of affected dogs – I fail to see the value of a scheme that actively perpetuates the very condition that it seeks to eliminate."
Dr. Rusbridge's and Ms. Knowler's second version of the protocol, which they published in August 2005, follows this presentation of the current, November 2006 third version, for comparison purposes. A major difference between the two versions is that the presence or absence of the Chiari-like malformation (CM) was dropped from the November 2006 breeding guidelines because of: (a) the ubiquity of the malformation within the CKCS population; (b) the lack of uniformity between veterinarians recognizing and consistently grading the severity of CM; and (c) the lack of evidence that the apparent severity of CM was related to severity of syringomyelia.
Introduction
The diagnosis of syringomyelia is easily confirmed by MRI but neurologists have yet to define what is meant by the term 'clear' given that most cavaliers have a degree of skull malformation. The late onset of clinical signs and the number of asymptomatic dogs adds to the complexity of the condition. Not enough is known about long term progression to ascertain the optimum age young dogs should be screened for the disease. The research is an evolving process and hopefully a proven accurate and UNIVERSAL scheme will be developed eventually. Recent studies suggests that in the vast majority of cases the syrinx starts in the upper cervical spinal cord so if this is included then scanning of the entire cord (more expensive) may not ultimately be necessary. Any 'normal' dog without the occipital malformation which makes the skull small has a genetic advantage and should be used for breeding.
The following breeding recommendations are made using current information and in response to breeder requests for guidelines. It has yet to be proven if this guide is appropriate. The aim of these recommendations is to reduce the incidence of symptomatic syringomyelia in the breed not to create litters of puppies guaranteed not to have SM as the chance of producing an affected dog cannot be predicted without knowing the inheritance. It is recommended that the offspring of any mating is also MRI screened before breeding. As the incidence of syringomyelia is so high in the breed there will be severe depletion of the gene pool if only clear dogs are used (i.e. other problems will develop). Therefore until the genetic defect is determined it is recommended that dogs with syringomyelia be used if they are valuable in another genetic sense e.g. good heart. The general principle of these guidelines is that dogs with code A are more desirable to use than B, etc but that dogs with a higher letter code may still be used in some limited circumstances.
RETURN TO TOP
International Syringomyelia Conference November 2006
Revised CKCS
MRI screening and breeding recommendations
These breeding recommendations are made using current information and in response to CKCS breeder request for guidelines. It has yet to be proven if this guide is appropriate. The aim of these recommendations is to reduce the incidence of symptomatic syringomyelia (SM) in the breed not to create litters of puppies guaranteed not to have SM as the chance of producing an affected dog cannot be predicted without knowing the inheritance.
Note- The age cut off at 2.5 years has been decided so as to tie in with MVD recommendations and because most dogs with symptomatic SM will show signs before 3 years of age.
The following categories from the previous guidelines [See August 2005 SM Breeding Recommendations, below] have been removed because of difficulty in accurately interpreting:
Previously A * - now A
Previously B - now C
Color code: red = under 2.5 years; blue = over 2.5 years; purple = any age
RETURN TO TOP
Results of Following Protocol
May 2021:
Summary of 2020 UK Kennel Club's 705 cavalier litters shows only 11 of 994
parents (0.01%) were tested for syringomyelia.
 Cassandra Smith has published her summary of the UK Kennel Club's
2020 breed records of cavalier King Charles spaniels. The summary is a
compilation of information from the CKCS litters registered with the
Kennel Club (KC), plus additional information from the KC's database,
including health testing statistics, as well as some independent
information garnered from Google searches. In the case of Chiari-like
malformation (CM) and syringomyelia (SM) data, she unfortunately has
combined official KC data using the BVA/KC CM/SM Screening Scheme with
possibly speculative information from outside official screening scheme
sources. Nevertheless, the results are disappointing:
Cassandra Smith has published her summary of the UK Kennel Club's
2020 breed records of cavalier King Charles spaniels. The summary is a
compilation of information from the CKCS litters registered with the
Kennel Club (KC), plus additional information from the KC's database,
including health testing statistics, as well as some independent
information garnered from Google searches. In the case of Chiari-like
malformation (CM) and syringomyelia (SM) data, she unfortunately has
combined official KC data using the BVA/KC CM/SM Screening Scheme with
possibly speculative information from outside official screening scheme
sources. Nevertheless, the results are disappointing:
• Only 4 of 705 litters (0.57%) had two MRI-screened parents, and of those 4, only 2 litters (0.28%) passed the breeding guidelines.
• Only 67 litters (9.5%) had public evidence (BVA/KC CM/SM Screening Scheme and/or Google) of one MRI-screened parent.
• 624 litters (89.9%) had no public evidence of either parent being MRI-screened.
• Only 11 parents (out of 299 sires and 695 dams = 994)(0.01%) were reported to have been screened under the BVA/KC CM/SM Screening Scheme.
• Of those 11 parents, 9 had CM (82%) and 1 had SM (9.1%).
• She reports that one dog with Grade 2 SM sired 3 litters in 2020.
January 2017: UK Kennel Club reports 2013-2014 compliance rate was 0.28%. In a report issued in November 2016, the UK Kennel Club announced:
"Looking at Kennel Club registration data reveals that only 0.28% of Cavalier King Charles Spaniel litters registered in 2013 and 2014 have come from parents that have both been BVA/KC graded."
October 2011: Effectiveness of SM breeding guidelines, and current statistics. In an October 2011 report [December 2011 hard-copy publication] of the effectiveness of the 2006 SM breeding recommendations and their current statistical results of following that SM protocol, the researchers, Dr. Rusbridge, Penny Knowler, and A. K. McFadyen stated that:
"This study investigated the early outcome of existing SM breeding guidelines. Six hundred and forty-three dogs, 550 Cavalier King Charles spaniels (CKCS) and 93 Griffon Bruxellois (GB), were identified as having either one (454 dogs) or both parents (189 dogs) with MRI-determined SM status.
• Offspring without SM were more common when the parents were both clear of SM (SM-free; CKCS 70 per cent, GB 73 per cent).
• Conversely, offspring with SM were more likely when both parents had SM (SM-affected; CKCS 92 per cent, GB 100 per cent).
• A mating of one SM-free parent with an SM-affected parent was risky for SM affectedness with 77 per cent of CKCS and 46 per cent of GB offspring being SM-affected. ...
"This paper serves to report the early outcome of using the 2006 breeding guidelines for dogs contributing to a genome project and whose pedigrees were known. The study suggested that SM-free offspring were more likely if both parents were SM-free and SM-affected offspring were more likely if both parents had SM. There was a trend that older SM-free dogs (*A) only resulted when at least one parent was *A. This finding seems logical but since *A and A grade dogs are in a minority it is problematic for breeders to select SM-free dogs especially when the SM status of the dog can alter with age. Often, the true SM status may not be known until after the dog is used for breeding. In 2010, there were 2136 CKCS litters registered with the UK kennel club (8095 puppies). Of these, 33 per cent had a sire aged younger than 2.5 years on the day of mating and 36 per cent had a dam younger than 2.5 years on the day of mating. This translates as 55 per cent of the KC registered CKCS puppies having one parent younger than 2.5 years and 14 per cent having both (Grahame Ford, personal communication). Thus, a recommendation that only A or *A grade parents be used is unlikely to be practical for breeders. If a younger SM-free dog (C grade) is mated with an older dog (A grade), then there is greater risk for SM than with two A grade parents. The data in the study (Tables 3 and 4) suggested that 63 per cent (12/19) of offspring were SM-free from A or*AxC parents. This is likely to be an overestimation of the proportion of SM-free dogs since these figures include C grade offspring, which may develop SM as they become older. However, it could be argued that a recommendation to include at least one A grade dog in any proposed mating is a reasonable, practical alternative since it allows breeders to use their younger dogs. However, a far better proposal for prevention of SM and maintaining genetic diversity is a proposed mate select programme using estimated breeding values (EBV). ...
"The most controversial part of the 2006 breeding recommendations was that it permitted older clinically asymptomatic SM-affected dogs to be bred to older SM-free dogs. This was because there were only a few A grade dogs identified when the breeding guidelines were first proposed and overuse of these might limit genetic diversity, reducing the effective population size. This investigation showed that a proportion of the offspring from such a cross can be SM-free, however, in the CKCS, the number of SM-affected dogs was far greater than SM-free dogs (77 per cent SM-affected). Moreover, where these offspring had siblings, the ratio of SM-free to SM-affected was 1:1 compared with 3.5:1 for *A or Ax*A or A parents or 1:1.7 for D or ExU parents (Knowler and Rusbridge, unpublished data). It is debatable whether it is ethical to knowingly breed a dog with an inherited disease especially when the majority of the offspring may be destined for the pet-owning public, and this study suggested that it is not advisable to use SM-affected dogs for breeding. However, if the prevalence of SM is as high as 70 per cent in the CKCS (Parker and others 2011), this will have dire consequences for the effective population size of the breed. Again it is hoped that using an EBV mate select programme may allow safer parental crosses, maintaining genetic diversity while decreasing the number of SM-affected offspring.
"One problem noted with the 2006 breeding guidelines was that if the dog was deemed asymptomatic but SM-affected when first scanned over 2.5 years old it was attributed a grade D status. However, in some cases it was suspected, due to the size of the syrinx, that if the dog had been scanned when younger then the syrinx would have been apparent, in other words, the dog was actually an E grade. It was also possible that some dogs may have been clinically affected (ie, an F grade) as the early behavioural signs of pain from SM and/or CM can be subtle and/or intermittent and may not be detected in a routine clinical examination. In addition, some breeders fail to recognise or acknowledge clinical signs of SM and/or CM. Since the aim of the guidelines is to reduce the incidence of early onset and clinical SM, a future recommendation is that a D status (or equivalent) will only be appropriate if the dog was first proved by MRI to be SM-free before 2.5 years of age. One encouraging observation was that the proportion of grade E (SM-affected younger than 2.5 years of age) dropped from an average of 15 dogs per year in years 2004 to 2006 to 11 dogs per year in years 2007 to 2009, that is, the breeding guidelines may be achieving the goal of reducing the risk of early onset SM, however, this hypothesis would be needed to be tested in a more vigorous study. ...
"In conclusion, the results from this study suggest that it is appropriate to continue using the breeding guidelines for both the CKCS and GB until a more robust system based on EBV or genetic testing is available. The following modifications are suggested but it should be realised that these are the recommendations that are based on limited data and consequently should be subjected to further prospective vigorous study:
• To increase the number of SM-free offspring, at least one parent should be ascertained to be SM-free by MRI as a young adult. In ideal circumstances, both parents would be SM-free. According to the study by Parker and others (2011), the optimum age for this early MRI screening is 36 months.
• If an SM-affected dog is used, for example, to preserve desirable traits or to increase genetic diversity then ideally the chosen mate would either be selected on the basis of its EBV and/or would be an older SM-free dog (five years or older).
• The offspring of the proposed mating should also be MRI scanned and ideally bred to older SM-free dogs.
• The SM status of the dog when at least five years old should be established. SM has a complex inheritance and an EBV mate select programme should allow breeders to select safer breeding combinations.
• To ensure success, the programme requires a substantial collection of accurate populationwide data. Consequently, all breeding dogs from breeds susceptible to CM and SM should be MRI screened and these results should be submitted to a central source.
• Pedigree and clinical history from dogs presenting with clinical signs of CM and/or SM should also be submitted to this central system. ‘D’ status (or equivalent) will only be appropriate if the dog was first proved to be SM-free before 36 months of age.
• Future breeding recommendations should also take account of dogs with CCD less than 2 mm. ..."
October 2010: Interim Statistics. In an October 2010 interim report of the statistical results of following the SM protocol, Dr. Rusbridge stated that:
(A) Offspring without SM only occurred when there was at least one parent of Grade A status;
(B) There were higher numbers of SM clear offspring it both parents had Grade A;
(C) All Grade A* offspring (SM clear over 5 years) had at least one parent that was Grade A*;
(D) 100% of offspring were SM affected if both parents were SM-affected;
(E) SM also occurs in Grade A x Grade A crosses (approximately 25%, but this figure might be improved if more older dogs are screened dogs);
(F) Using dogs of unknown status was risky for SM affectedness;
(G) 50% of dogs in a Grade A x Unknown cross were SM affected.
*Note: Grade A* means that the dog had no SM at all and no CM at all.
Dr. Rusbridge provided these interim statistics:
● Matings of Code A CKCS to Code A CKCS have produced 75.9% offspring with no SM.
● Matings of Code A CKCS to either Code D, E, or F CKCS have produced 41.9% offspring with no SM.
● Matings of Code A CKCS to unscanned CKCS have produced 50.0% offspring with no SM.
● Matings of Code D CKCS to Code D, E, or F CKCS have produced no offspring free of SM.
RETURN TO TOP
August 2005 Version of the Syringomyelia Breeding Protocol
The following is the August 2005 protocol by Dr. Rusbridge and Ms. Knowler. As their research has progressed and their knowledge of the disease has increased, they have modified their earlier recommendations.
What follows, first, is their verbatim August 2005 Syringomyelia Breeding Protocol, followed by the CavalierHealth.org editor's analysis of their breeding recommendations. To best understand the terminology which they use, the reader first should read Syringomyelia In Depth. All Cavalier fanciers should be deeply indebted to these SM researchers and their counterparts worldwide for the effort they have put into assisting CKCS breeders in taking measures to reduce the incidence of SM in future generations of the breed. Of course, it is completely up to the breeders as to whether they will pay any attention at all to these guidelines.
Rusbridge/Knowler Syringomyelia Breeding Recommendations
(August
2005)
by Dr. Clare Rusbridge and Susan P. (Penny) Knowler
The diagnosis of syringomyelia is easily confirmed by magnetic resonance imaging (MRI), but neurologists have yet to define what is meant by the term “clear”, given that most Cavaliers have a degree of skull malformation. The late onset of clinical signs and the number of asymptomatic dogs adds to the complexity of the disease. Not enough is known about long term progression to ascertain the optimum age young dogs should be screened for the disease. The research is an evolving process, and hopefully a proven accurate and UNIVERSAL scheme will be developed eventually. Recent studies suggest that in the vast majority of cases, the syrinx starts in the upper cervical spinal cord, so if this is included, then MRI scanning of the entire spinal cord (more expensive) may not ultimately be necessary. Any “normal” dog, without the occipital malformation which makes the skull small, has a genetic advantage and should be used for breeding.
The following breeding recommendations are made using current information and in response to breeder requests for guidelines. It has yet to be proven if this guide is appropriate. The aim of these recommendations is to reduce the incidence of symptomatic syringomyelia in the breed -- not to create litters of puppies guaranteed not to have SM -- as the chance of producing an affected dog cannot be predicted without knowing the inheritance. It is recommended that the offspring of any mating is also MRI screened before breeding. As the incidence of syringomyelia is so high in the breed, there will be severe depletion of the gene pool if only clear dogs are used (i.e. other problems will develop). Therefore, until the genetic defect is determined, it is recommended that dogs with syringomyelia be used if they are valuable in another genetic sense (e.g. good heart). The general principle of these guidelines is that dogs with Grade A are more desirable to use than those with Grade B, etc., but that dogs with a higher letter Grade may still be used in some limited circumstances.
Notes: The age cut off at 2.5 years has been decided so as to tie in with MVD recommendations and because most dogs with symptomatic syringomyelia will show signs before 3 years of age. These recommendations will only work if the Cavaliers are actually MRI scanned!! Any dog not MRI scanned is assumed to be Grade D or E depending on its age. Dogs may develop signs of syringomyelia at any age, e.g., a dog can be free of pain until 7 years old, i.e. , a dog’s status may change as it gets older.
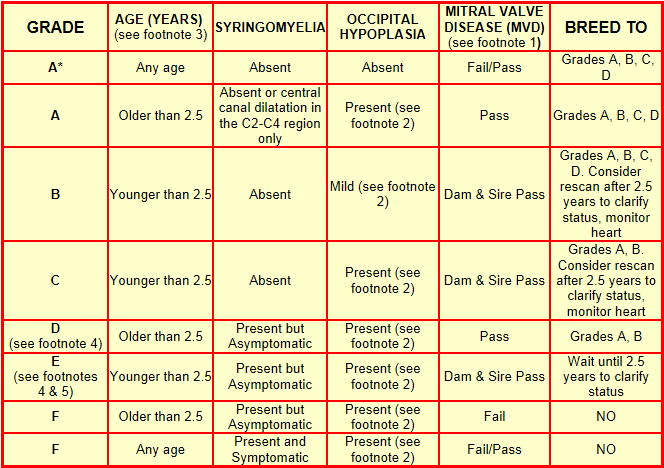
Footnotes to Table:
1. MVD - to "Pass", a Cavalier must be free of systolic murmur over 2.5 years old with systolic murmur-free parents over 5 years old. [Editor's Note: This is the MVD Breeding Protocol.]
2. Occipital hypoplasia can be difficult to define because, in comparison to other toy breeds, the back of the CKCS's skull is smaller – i.e.‚ a "normal" Cavalier skull is very hard to find, and there are few CKCS that meet Code A+. In addition, the term "too small" has not been defined; nor is there a consensus as how to measure the occipital bone. Basically, there are three classic features of occipital malformation: (1) loss of the normal round shape of the cerebellum, which can appear indented by the occipital bone; (2) displacement of the cerebellum into and through the foramen magnum, i.e., herniation; and (3) kinking of the medulla. Mild occipital hypoplasia is defined as a displacement of the cerebellum into the area of the foramen magnum and slight kinking of medulla and indentation of the cerebellum (see diagrams below).
 Mild occipital hypoplasia –
[right] The cerebellum is very slightly
indented. The kinking of the medulla is normal for a toy breed, and
there is displacement of the cerebellum into and just out of the foramen
magnum. The ventricular system is slightly dilated. This dog is Grade B.
If he was older than 2.5 years, he would be Grade A.
Mild occipital hypoplasia –
[right] The cerebellum is very slightly
indented. The kinking of the medulla is normal for a toy breed, and
there is displacement of the cerebellum into and just out of the foramen
magnum. The ventricular system is slightly dilated. This dog is Grade B.
If he was older than 2.5 years, he would be Grade A.
 Although the cerebellum is not coming through the foramen magnum,
this dog [right] has a greater degree of occipital hypoplasia than the
dog above. See how the cerebellum is indented and the medulla is kinked.
The central canal is dilated above the first disc space – this is the
first sign of syringomyelia developing. There is also mild ventricular
dilatation. This dog would be Grade C if less than 2.5 years.
Although the cerebellum is not coming through the foramen magnum,
this dog [right] has a greater degree of occipital hypoplasia than the
dog above. See how the cerebellum is indented and the medulla is kinked.
The central canal is dilated above the first disc space – this is the
first sign of syringomyelia developing. There is also mild ventricular
dilatation. This dog would be Grade C if less than 2.5 years.
 This dog
[right] has descent of the cerebellum towards the foramen
magnum and the cerebellum is indented. The medulla is normal for a toy
breed; there is mild ventricular dilatation and a small syrinx/central
canal dilatation in the upper cervical spinal cord. However he is 8
years old with a clear heart. He is Grade A.
This dog
[right] has descent of the cerebellum towards the foramen
magnum and the cerebellum is indented. The medulla is normal for a toy
breed; there is mild ventricular dilatation and a small syrinx/central
canal dilatation in the upper cervical spinal cord. However he is 8
years old with a clear heart. He is Grade A.
3. Dogs may develop signs of syringomyelia at any age, e.g., a dog can be free of pain until 7 years old. Therefore, a dog’s status may change as it gets older.
4. Any dog not MRI scanned is assumed to be no better than Grade D or E, depending upon its age.
5. Breed clubs should consider whether to recommend that stud dogs are MRI scanned. Males have most influence on the gene pool (popular champions sire hundreds) and by the time it is known that a dog may pass on the tendency, his genes may be widespread. It would be sensible that if a male dog is to be used more than twice, then, for the safety of the breed, he should be Grade A or B. It would perhaps be a good use of research funds to use them to subsidize the testing of stud dogs and publish a clear list. A salient fact is that 93% of the top stud dogs in the UK are closely related to one or more dogs with SM, and the pedigrees of these dogs are similar to champions worldwide.
RETURN TO TOP
Editor's Analysis of Rusbridge/Knowler August 2005
Syringomyelia
Breeding Recommendations
The latest version of the syringomyelia (SM) breeding protocol raises several significant points:
First, all grades of Cavaliers to be bred under this protocol (Grades A*, A, B, C, and D) should have been examined by an MRI scan. Under previous SM protocols, Rusbridge/Knowler expressly allowed for breeding certain CKCSs which had not been scanned. They state here that any un-scanned Cavalier is to be graded D or E, depending upon its age.
The ideal candidate for breeding is graded A*, which is a Cavalier which qualifies under the mitral valve disease (MVD) breeding protocol and has neither SM nor occipital hypoplasia. A Grade A* Cavalier may be bred to any of the lower grade dogs, A, B, C, and/or D.
It is obvious that Rusbridge/Knowler do not believe that there will be enough breedable Cavaliers which are Grade A*, because they then list lower grades (A, B, C, and D), all of which either have occipital hypoplasia with no SM or even have mild forms of SM.
Despite all CKCSs having MRIs, Rusbridge/Knowler's second category, Grade A, allows for the breeding of Cavaliers which have been diagnosed with both occipital hypoplasia and a mild case of SM. Grade A dogs are over age 2.5 and have satisfied the MVD breeding protocol but which may have a form of SM, central canal dilatation of the spinal cord, in the C2-C4 region of the spine. These Grade A Cavaliers may be bred to Grade A, B, C, and/or D dogs.
Rusbridge/Knowler's third level of eligible CKSCs are those under age 2.5 years and diagnosed with occipital hypoplasia but no SM. These are dogs graded B (mild occipital malformation) or C (the malformation is "present"). Significantly, the breeding of CKCSs in this category would violate the MVD breeding protocol, since that protocol forbids breeding any Cavalier under age 2.5 years. Rusbridge/Knowler temper their recommendation of breeding a Grade B or C dog by requiring that the both of the dog's parents meet the MVD protocol by being MVD-murmur clear at age 5 years. So, under the Grade B and C categories, if the breeding dog's parents satisfy the MVD protocol, it may be bred even though it is under age 2.5 years.
The Grade B Cavalier, which has only mild occipital hypoplasia, may be bred to any grade of Cavalier: A, B, C, and/or D. The Grade C Cavalier, with occipital hypoplasia "present" (and presumably more severe than just "mild") may be bred only to Grade A or B dogs. Rusbridge/Knowler recommend that both Grade B and C Cavaliers be re-scanned with MRI after age 2.5 years, and that the MVD status continue to be monitored.
Rusbridge/Knowler do not appear to explain why they believe it appropriate to breed any Cavalier under age 2.5 years. The MVD breeding protocol is emphatic that no CKCS be bred under age 2.5 years, so as to reduce the incidence of early-onset MVD. Perhaps Rusbridge/Knowler have weighed the risk of perpetuating early-onset MVD against any onset of SM. Granted, even these underaged CKCSs must have parents which had clear hearts at age 5 years. So, they are heeding some aspects of the MVD protocol. But they still do not appear to answer the obvious questions: Why not wait until the Grade B and C breeding stock is 2.5 years old and MVD murmur-free? What is their scientific basis for the rush?
These underaged Grade B and C Cavaliers clearly are not ideal candidates for breeding, because, as Rusbridge/Knowler note in their recommendations, the first MRI evidence of SM may not show up until age 2.5 years or older.
Their next category of breedable Cavalier, Grade D, is over age 2.5 years, meets the MVD protocol, but has both the occipital malformation and asymptomatic SM (SM without any symptoms).
Finally, they list two categories of non-breedable Cavaliers, Grades E and F. A Grade E dog is under age 2.5 years, with parents who meet the MVD protocol, but which has both the malformation and asymptomatic SM. Instead of breeding the underaged Grade E Cavalier now, they recommend waiting until it is over 2.5 years. Presumably then, if it passes the MVD protocol, it will become a breedable Grade D, and if it fails the MVD test, it will be a non-breedable Grade F.
The Grade F Cavalier can be in either of two sub-categories. Neither makes it breedable. It can be over age 2.5 and not meet the MVD protocol, with both the occipital malformation and asymptomatic SM. Or it can be of any age, either pass or fail the MVD protocol, and have symptomatic SM.
As for the vast majority of Cavaliers, those which are un-scanned, Rusbridge/Knowler grade them either D or E, depending upon their ages. Of course, an un-scanned Cavalier with symptomatic SM would have to be Grade F, although Rusbridge/Knowler do not expressly say that.
In conclusion, Rusbridge/Knowler's August 2005 SM breeding recommendations align tightly, although not exclusively, with the MVD breeding protocol. In two instances, Grades B and C, they allow for underaged Cavaliers to be bred, but they require the parents to pass the MVD protocol (meaning be murmur-clear at age 5 years), and they advise that the Cavaliers' hearts be monitored and re-examined after age 2.5 years. All in all, the August 2005 Rusbridge/Knowler SM breeding protocol is a refreshing and robust re-affirmation of the 1998 MVD breeding protocol. Let us hope that more CKCS breeders start paying heed to it, as well.
RETURN TO TOP
Related Links
RETURN TO TOP
Veterinary Resources
Interim Breeding Guidelines -- 4 Year Report. SP Knowler, AK McFadyen, C Rusbridge. Abstract at 23d ECVN symposium, Sept. 2010. Quote: ...a cohort of 465 dogs (307 females, 158 males) were identified which had either one (316 dogs) or both parents (149 dogs) with MRI confirmed CMSM status. Of these, 393 were CKCS [cavalier King Charles spaniels] and 72 were Griffon Bruxellois. All dogs were assigned an A - F CMSC grade according to the current breeding guidelines. Grade A implies a SM unaffected dog over 2.5 years old. In addition, to estimate the influence of late onset SM, an Grade A* was assigned to Grade A dogs over 5 years old. The CMSM grade of all offspring from all possible breeding combinations including using one parent of unknown status (Grade U) was ascertained. Offsrping without SM only occurred when there was at least one parent of Grade A status. There were higher numbers of SM clear offspring if both parents had A status. In addition all A* offspring also had at least one A* parent and higher numbers of A* offspring resulted from crosses where both parents were A*. There was no influence of gender on SM affectedness. All offspring were SM affected if both parents were SM affected. SM affected offspring may also occur when SM unaffected dogs are used (15.4% from A x A parent crosses and 7.7% from A* x A* parental crosses). Using dogs of unknown status was risky for SM affectedness. Fifty percent of older offspring were SM affected in A x U parental crosses and there were higher numbers of SM affected dogs with other parental combinations that included one Grade U dog. In conclusion, to increase the number of SM unaffected offspring, at least one parent should be ascertained to be free of SM by MRI at 2.5 years of age. Ideally both parents would be free of SM at 2.5 years of age and the true SM status of the grandparents at least 5 years old should be established. It is recommended that all breeding dogs from breeds susceptible to CMSM be MRI screened and results submitted to an officially recognised central database.
Growth of Clinical Veterinary Magnetic Resonance Imaging. Patrick R. Gavin. Vet.Rad. & Ultra.; Mar/Apr 2011; 52(s1):52-54. Quote: In the spine, MR imaging reveals conditions which were previously difficult to diagnose ante-mortem, and may facilitate study of their pathophysiology. Examples include syringohydromyelia associated with Chiari-like malformation in the Cavalier King Charles spaniel... .
Prevalence of asymptomatic syringomyelia in Cavalier King Charles spaniels. J. E. Parker, S. P. Knowler, C. Rusbridge, E. Noorman, N. D. Jeffery. Vet.J. June 2011. Quote: The prevalence of syringomyelia was investigated in a sample population of 555 Cavalier King Charles spaniels. All dogs, which were declared by their owners to be showing no clinical signs of syringomyelia, underwent MRI to determine the presence or absence of the condition. Data were analysed by logistic regression to determine the effects of sex and age on the prevalence of syringomyelia. Only increased age was found to have a significant effect. The prevalence of syringomyelia was 25 per cent in dogs aged 12 months, increasing to a peak of 70 per cent in dogs aged 72 months or more. ... The evidence for a lower prevalence in younger animals is more reliable (because of the higher numbers included in the present study and the lower likelihood of false inclusion) and this effect lasts until dogs are at least three years of age. This finding has important implications for the design of a screening test procedure and may conflict with the current recommendations that the optimum age for screening should be 30 months. These data would imply that it is probable that dogs aged up to three years may yet have reduced odds for the diagnosis of syringomyelia. However, there is a need for the dogs to be screened when they are reasonably young so that breeders can decide at an early stage whether their animals are suitable for breeding; many breeders would consider 36 months unduly old.... The high lifetime prevalence of syringomyelia raises concerns for the welfare of the CKCS breed and also suggests that eliminating the genetic risk factors for the disease by selective breeding may be difficult, because the heritability has previously been shown to be complex, and the prevalence of the determinant genes within the population is therefore likely to be high. The true prevalence of syringomyelia in the general CKCS population is expected to be higher than that found in this sample population because symptomatic dogs were specifically excluded.
Effectiveness of breeding guidelines for reducing the prevalence of syringomyelia. S. P. Knowler, A. K. McFadyen, C. Rusbridge. Vet Rec Oct 2011; doi:10.1136/vr.100062; Vet Rec Dec 2011;169:679-680. Quote: Several toy breed dogs are predisposed to syringomyelia (SM), a spinal cord disorder, characterised by fluid-filled cavitation. SM is a complex trait with a moderately high heritability. Selective breeding against SM is confounded by its complex inheritance, its late onset nature and high prevalence in some breeds. This study investigated the early outcome of existing SM breeding guidelines. Six hundred and forty-three dogs, 550 Cavalier King Charles spaniels (CKCS) and 93 Griffon Bruxellois (GB), were identified as having either one (454 dogs) or both parents (189 dogs) with MRI-determined SM status. Offspring without SM were more common when the parents were both clear of SM (SM-free; CKCS 70 per cent, GB 73 per cent). Conversely, offspring with SM were more likely when both parents had SM (SM-affected; CKCS 92 per cent, GB 100 per cent). A mating of one SM-free parent with an SM-affected parent was risky for SM affectedness with 77 per cent of CKCS and 46 per cent of GB offspring being SM-affected. It is recommended that all breeding dogs from breeds susceptible to SM be MRI screened; that the SM status at five years old is established; and all results submitted to a central database that can be used by dog breeders to better enable mate selection based on estimated breeding values.
Can breeding strategies modify or eliminate the syringomyelia phenotype? Colin J. Driver, Holger A. Volk. Vet Rec Dec 2011;169:679-680.
CONNECT WITH US